Presumptive Eligibility Guide
Printing the manual material found at this website for long-term use is not advisable. Department Policy material is updated periodically and it is the responsibility of the users to check and make sure that the policy they are researching or applying has the correct effective date for their circumstances.
If you experience any difficulty opening a section or link from this page, please email the webmaster.
Return to the Presumptive Eligibility Page
How to Search this manual:
This edition has three search options.
- Search the whole guide. Open the Complete Manual tab. From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials".) The search box will show all locations where denials are discussed in the manual.
- Search by chapter. Open any chapter tab (for example the "Billing Procedures" tab). From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials".) The search box will show where denials are discussed in just that chapter.
- Site search. Search the guide as well as other documents related to a particular search term on the Montana Healthcare Programs site specific search page.
Prior guides may be located through the provider website archives.
Updated 06/30/2026
Presumptive Eligibility Qualified Entity Reference Guide
To print this manual, right click your mouse and choose "print". Printing the manual material found at this website for long-term use is not advisable. Department Policy material is updated periodically and it is the responsibility of the users to check and make sure that the policy they are researching or applying has the correct effective date for their circumstances.
Update Log
Publication History
This publication supersedes all previous Presumptive Eligibility. Published by the Montana Department of Public Health & Human Services, July 2016 and prior. This manual was updated June 2017.
CPT codes, descriptions and other data only are copyright 2014 American Medical Association (or such other date of publication of CPT). All Rights reserved. Applicable FARS/DFARS Apply.
Update Log
06/15/2017 The manual was updated to include 2017 requirements and converted to a 508 compliant format.
Table of Contents
Presumptive Eligibility Public Assistance Programs
Key Contacts
Definitions
The Role of a Qualified Entity
Eligibility and Coverage
Timing
Step 1 – Verify the Person(s) Coverage Status
Step 2 – The Presumptive Eligibility Application
Applicant Information
Household Information
Income Information and Signature
Application Addendum for Immigrants (Information on Qualified Non-Citizens)
QE Evaluates Who Counts in Household Size
Step 3 – Making a PE Determination
Step 4 – Evaluate for Community Engagement Requirements
Step 5 – Finalizing the PE Process
Provide Applicant with Information and Proof of Temporary Coverage
Step 6 – Follow Up and Scan/Fax
Summary of Qualified Entity Responsibilities
Key Contacts:
Please contact us at any time if you have questions, need training or additional supplies, or need to verify any information about presumptive eligibility.
Presumptive Eligibility Public Assistance Programs
Beginning January 1, 2014, hospitals and other designated facilities participating with Medicaid can offer Presumptive Eligibility (PE) to additional coverage groups.
Note: Prior to 2014, PE was available only for children and pregnant women. PE is now available for additional Medicaid coverage groups for individuals who meet eligibility requirements. The following Medicaid coverage groups may receive Presumptive Eligibility if they meet eligibility requirements.
All providers electing PE must comply with State of Montana requirements for determining PE for the following groups:
► HMK Plus, formerly known as Children’s Medicaid
- Children 0 up to age 19
- Income limits up to 143% Federal Poverty Level
- Children may have primary insurance and still qualify for HMK Plus
► HMK, formerly known as Children’s Health Insurance Program (CHIP)
- Children 0 up to age 19
- Income limits up to 261% Federal Poverty Level
- Applicants CANNOT have other health insurance and receive HMK
► Parent/Caretaker Relative (Medicaid)
- For individuals who live together and are related by Marriage and/or Parentage.
- The parent or caretaker relative must have a related dependent child under age 19 living with them in the home to be eligible.
► Pregnant Woman
- Must be pregnant at the time of application and have income at or below 157% of the FPL
- A pregnant woman may be eligible for PE more than once in 12 months if they are pregnant more than once in that 12- month period
- For Pregnant women presenting for services prior to delivery
- See Income Calculation Tool for Household Income levels
► Individuals age 19-64 (Medicaid Expansion)
- For individuals between the ages of 19-64.
- Not pregnant at the time of application.
- Not eligible for or enrolled in Medicare Part A
- Not enrolled in Medicare Part B
- For parents and caretakers not income eligible for the Parent/Caretaker Relative Medicaid.
- Individuals may need to be evaluated for Community Engagement requirements if they meet Medicaid Expansion eligibility criteria, and do not qualify for an exclusion.
► Former Foster Care (Medicaid)
- Adults 19 up to 26
- For individuals who were in Foster Care and receiving Medicaid when they turned 18
- No income limit or resource/asset test
- Should be evaluated for PE as an individual even if living in a household with other family member
► Breast and Cervical Cancer
- For woman (ages 19 through 64) presenting for services after screening at a designated Montana Breast and Cervical Health Program facility AND after receiving diagnosis and treatment options for breast and/or cervical cancer.
- The following forms must be presented to be eligible for PE:
- Montana Breast and Cervical Screening Form
- Enrollment Form, and
- Montana Breast and Cervical Cancer Treatment Program Medicaid Referral
- Income and household size do not need to be evaluated for PE since they are reviewed during the Breast and Cervical Cancer Screening process.
- Applicants cannot have other insurance which covers breast or cervical cancer treatment.
Benefits for each of these groups vary according to the coverage group. Presumptive eligibility provides immediate, temporary health coverage for eligible individuals. Recipients are allowed ONE PE period every 12 months (dated from the most recent PE effective date) OR once per pregnancy. (A pregnant woman may be eligible more than once in 12 months if they have more than one pregnancy during that 12-month period).
Definitions:
Applicant:
Person applying for coverage for themselves, a spouse, or dependent child
Application:
The Presumptive Eligibility Application
Application for Health Coverage:
The “Application for Health Coverage & Help Paying Costs” used to apply for ongoing health coverage for Medicaid, HMK, or HMK Plus. Appendices A, B, or C may need to be completed if they apply.
Breast and Cervical Cancer:
Women ages 19 through 64 who have been screened and diagnosed with breast or cervical cancer; applicants must present 3 required forms and must not have other insurance which covers cancer treatment.
Determination:
Eligibility decision for Presumptive Eligibility (PE) coverage.
Determination Date:
The date a presumptive eligibility decision is made by a Qualified Entity (QE).
Eligibility Period:
Presumptive Eligibility coverage starts on the date of determination and ends the earlier of: the date a determination of ongoing program eligibility is made, or the end of the month following the month of the PE determination. An applicant may have only one PE period in 12 months, or only one PE Period per pregnancy.
Federal Poverty Level (FPL):
Poverty guidelines for the 48 contiguous stated and the District of Columbia as published under the “Annual Update on HHS Poverty Guidelines” in the Federal Register each year, on or about February 15. The FPL is used in combination with household size to determine presumptive eligibility.
Former Foster Care between ages 18 and 26: Individuals who were in Foster Care and receiving Medicaid when they turned 18. May apply for PE if between ages 18 and 25(until age 26), and should be evaluated for PE as an individual even if living in a household with other family members. No Income limits apply.
Health Montana Kids (HMK):
Formerly known as the "Children’s Health Insurance Plan(CHIP)", HMK serves eligible children up to age 19 in households with income between 143% and 261% of the FPL.
Health Montana Kids Plus (HMK Plus):
Formerly known as "Children’s Medicaid", HMK Plus serves eligible children up to age 19 in households with incomes between 0% and 143% of the FPL.
Income Calculation Tool:
Reference table identifying household size and corresponding maximum income levels for persons or households applying for Presumptive Eligibility.
Individuals ages 19-64:
This expansion group covers individuals ages 19-64 that are not pregnant at the time of application, not eligible for or enrolled in Medicare Part A, not enrolled in Medicare Part B and are between 24% and 133% of the FPL.
Parent/Caretaker Relative Medicaid:
For individuals living together and related by marriage and/or parentage. The parent or caretaker relative must have an eligible related dependent child under age 19 living in the home and have income between 0% and 23% of the FPL.
Pregnant Woman:
Pregnant women presenting for services prior to delivery. The income limit for this category is from 0% to 157% of the FPL. No hard copy verification of pregnancy is required. Covers ambulatory prenatal care ONLY.
PE Determination:
A decision of temporary eligibility is called a determination. A Qualified Entity (QE) from a healthcare facility must be trained by the State of Montana in order to make a PE Determination based on self-attested information provided by an individual or household.
Presumptive Eligibility (PE): Expedited eligibility process of determining temporary health care coverage for persons eligible for specific public assistance programs.
Proof of Temporary Coverage Letter:
Approval notices prepared by a QE verifying temporary coverage in a specific public assistance program; used in place of a member ID card.
Qualified Entity (QE):
Representative of a health facility trained and certified to make Presumptive Eligibility determinations.
Self-Attestation:
An applicant’s sworn statement of the accuracy of the information they provide, such as income, household size, and residency, as reported on an application or as a change either verbally, electronically, or in writing.
Web Portal:
On-Line resource site for Qualified Entities and health care providers to check current health care coverage for persons applying for PE ( access from the home page of the provider website).
The Role of a Qualified Entity
Access to health care is critical for uninsured or underinsured persons when faced with sudden, serious, and often very expensive health care needs. Qualified Entities are vital to the Presumptive Eligibility process. As a Qualified Entity, you are trained and certified to make accurate, complete and timely determinations of PE coverage. PE begins on the date a Qualified Entity makes a PE determination and continues until a complete eligibility determination is made or until the last day of the month following the month PE began, whichever occurs first. Reimbursement for your facility, and the family’s peace of mind depend upon your due diligence and attention to detail. Once you determine a person presumptively eligible, your facility’s services will be paid covered services on or after the date of your determination, and PE coverage may continue for a period up to the end of the month following the month of determination. If a PE application was turned in for a group that is not eligible for PE coverage, they would be denied, and the client would be responsible for the services they received. This is yet another reason to have the client complete a regular Medicaid application.
Eligibility and Coverage
- Presumptive Eligibility is based primarily on age, status of the applicant(s), and household size and income.
- PE Coverage is temporary – Eligibility begins on the date of determination and ends the last day of the month following the month of determination, or sooner, if a determination of ongoing program eligibility is finalized. Facilities are required to provide applicants with the Application for Coverage and Help Paying Costs and Appendices A, B, and C , and assist with the completion of applications and appendices if necessary.
- A person may have only ONE PE period in a twelve month period, OR once per pregnancy. (A pregnant woman may be eligible more than once in 12 months if they have more than one pregnancy during that 12-month period).
- Presumptively eligible persons receive the same benefits as a standard covered enrollee in the public assistance program for which they are eligible during the presumptive eligibility period. The exception to this is Pregnant Woman Presumptive, only ambulatory services are covered.
Timing
- On the date a person presents for services, or as soon as possible, have the applicant (or a representative) complete the Presumptive Eligibility Application. PE coverage begins on the date of determination . If eligible, the person has timely coverage, and the facility is reimbursed for covered services.
- The PE application AND the Proof of Temporary Coverage Form must be faxed or scanned and emailed to the Human and Community Services Central Office within 5 days of making the Presumptive Eligibility Determination. Staff will then finalize the PE enrollment so eligibility information displays correctly on the web portal to generate the appropriate reimbursement for services.
- If a PE determination cannot be made on the date a person presents for services or the first day of a hospital stay, an Application for Health Coverage and Help Paying Costs should be completed an turned in to the State (with required documentation) during the same month the person receives series. Then, pending an eligibility determination, the eligibility effective date would be the 1st of the month of application OR date of birth (for newborns).
Step 1 - Verify the Person(s) Coverage Status
* Verify if the person has current coverage and/or
* Verify if the person has received Presumptive Eligibility within the past 12 months:
► Web Portal – www.mtmedicaid.org (see “Eligibility Spans”, example below)
► Fax Back – 1-800-714-0075
► Automated Voice Response – 1-800-714-0060
Web Portal Example 1 (Verify if the person has current coverage):

Web Portal Example 2 (Verify if the person had PE within the past 12 months):

 are not eligible for PE, but the \"Application for Health Coverage\" should be offered. A pregnant woman may be eligible for PE more than once in 12 months if they are pregnanat more than once during that 12-month period.")
Step 2 – The Presumptive Eligibility Application
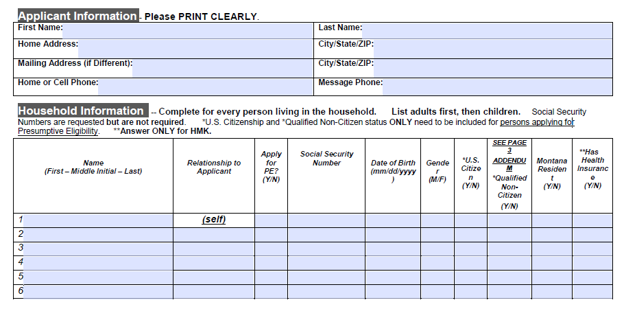
Have the Applicant (or a representative) complete the Presumptive Eligibility Application as follows:
-
Applicant and Household Non-financial Information
-
Household Information
►Page 3 of the application also includes an Addendum for immigrants who need information about whether they are a Qualified Non-Citizen. The Addendum does not need to be submitted with the PE application. See the information from the Addendum later in this chapter.
►"Has Health Insurance" applies only to those who may qualify for HMK PE
-
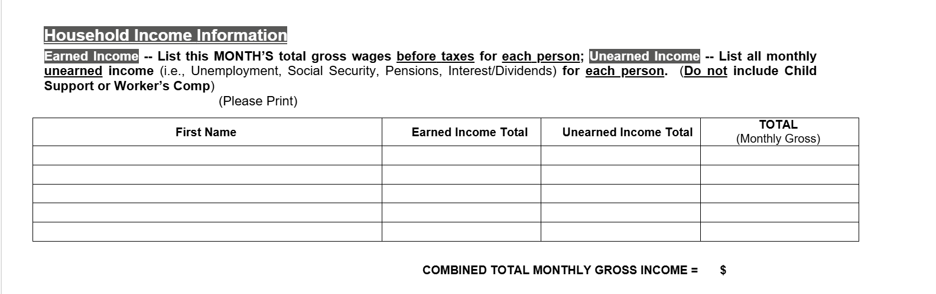
Income and Signature
-
Application Addendum for Immigrants (Information on Qualified Non-Citizen)
ALL PERSONS WHO ARE IMMIGRANTS NEED TO REVIEW THE FOLLOWING INFORMATION TO DETERMINE IF THEY ARE A QUALIFIED NON-CITIZEN; THEN THEY SHOULD MARK THE APPROPRIATE RESPONSE ON THE
PRESUMPTIVE ELIGIBILITY APPLICATION, HOUSEHOLD INFORMATION, COLUMN 8.
Those who are in ANY of the following groups would be considered a Qualified Non-Citizen:
- Lawful Permanent Residents (LPR/Green Card Holder ) **SEE FURTHER INFORMATION, BELOW
- Asylees
- Refugees
- Cuban/Haitian entrants
- Paroled into the U.S. for at least one year
- Conditional entrant granted before 1980
- Battered non-citizens, spouses, children, or parents
- Victims of trafficking and his or her spouse, child, sibling, or parent or individuals with a pending application for a victim of trafficking visa
- Granted withholding of deportation
- Member of a federally recognized Indian tribe or American Indian born in Canada
- Children lawfully residing in the state of Montana (lawfully present and otherwise eligible for Medicaid or HMK in the state, including being a state resident)
**In order to get Medicaid coverage, under current law most ADULT Lawful Permanent Residents or green card holders have a 5-year waiting period. This means they must wait 5 years after receiving “qualified” immigration status before being eligible for Medicaid. There are also exceptions -- Lawful Permanent Residents who don’t have to wait 5 years -- such as people who used to be refugees or asylees.
Montana has removed the 5-year waiting period to cover lawfully residing children who are otherwise eligible for Medicaid or HMK. A child is “lawfully residing” if lawfully present and otherwise eligible for Medicaid or HMK in the state (including being a state resident).
NOTE: Immigrants who are qualified non-citizens are generally eligible for Medicaid and Children’s Health Insurance Program (HMK) coverage IF they are otherwise eligible for Medicaid and HMK in the state; that is, if they meet Montana’s income eligibility rules .
-
QE Evaluates Who Counts in Household Size
Before making a PE Determination, a Qualified Entity needs to evaluate which individuals will be “counted” as part of the household. The following examples can be referenced for how to count persons in the household.
Pregnant Women: Include the pregnant woman, the unborn child(ren), the father of the unborn (if married and living together), and any other children (of the unborn’s married parents) under age 19 who live in the home. For example:
- Ann is a single mother with one child and has a significant other in the household. She is pregnant with one child. For this household,
Count: Ann, her child, and the unborn (Household Size 3). Do not count the significant other OR his income because he and Ann are not married. - Julie and her husband are expecting their first child, and are living in the same household.
Count: Julie, her husband, and the unborn (Household size 3) and all their income. - Mary and her husband have 2 children and Mary is pregnant. They currently live with Mary’s parents, who require living assistance.
Count: Mary, her husband, their 2 children and the unborn (Household size 5) and their income.
DO NOT Count Mary’s parents.
Healthy Montana Kids (HMK), Health Montana Kids Plus (HMK Plus), Parent/Caretaker Relative, and individuals between 19-64 years old: Include all those on the application that are connected by marriage or parentage who live in the household, along with any unborn children. This includes all Natural, Adoptive, and/or Step-Parents and birth, adoptive, or step-children under age 19, as well as any unborn children of these persons. DO NOT INCLUDE other adult relatives who file their own tax return. For Example:
- Pamela, her significant other Dan, Pamela’s two children, and Pamela and Dan’s unborn child all live together.
Count: Pamela, her two children, and the unborn (Household size 4).
DO NOT Count: Dan and his income until there is a child in common for him and Pamela. Once the baby is born, Count: Pamela, Dan, her two children, and Pamela and Dan’s child in common (Household Size 5), as Dan is connected by parentage. - Lily, Rose, and Paul live with their maternal grandparents and are not adopted by the grandparents.
Count: Lily, Rose, and Paul only (Household size 3).
Do Not Count: The grandparents as they are not related by parentage. - Susan has 3 children, including and 18 year old daughter who just had a baby. Susan’s brother Michael and his son also live with Susan, her children and grandchild.
Count: Susan, her children, and her grandchild (Household Size 5).
Do Not Count: Michael and his son don’t count as they are not related to Susan, her children or grandchild by marriage or parentage.
Individuals age 19-64 : Include all household members that are between the ages of 19 and 64, not pregnant at the time of application, not eligible for or enrolled in Medicare Part A or B, and Parent/Caretaker relatives that are over income for the Parent/Caretaker Relative Medicaid. For Example:
- Cindy, her significant other Jim, and her two children all live together.
Count: Cindy and her two children.(Household Size 3).
Do Not Count: Jim is his own household. Because Cindy and Jim are not married, they will not be counted in the same household. If they were married, everyone would be included (Household size 4).
Step 3 – Making a PE Determination
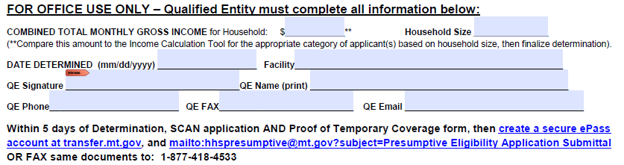
Qualified Entities must complete the “For Office Use only” box for ALL PE Determinations.
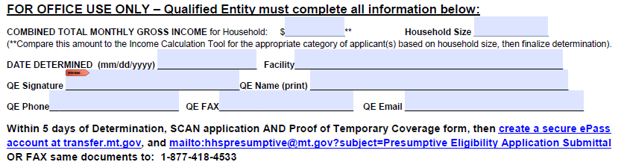
Complete the entire box “For Office Use Only.” Copy the “Combined Total Monthly Gross Income” figure from the applicant’s Income information box. Count how many people are in the household and record the number under “Household Size” in the box shown above. Compare Combined Total Monthly Gross Income to Current Income Calculation Tool based on household size for the program being considered for each individual.
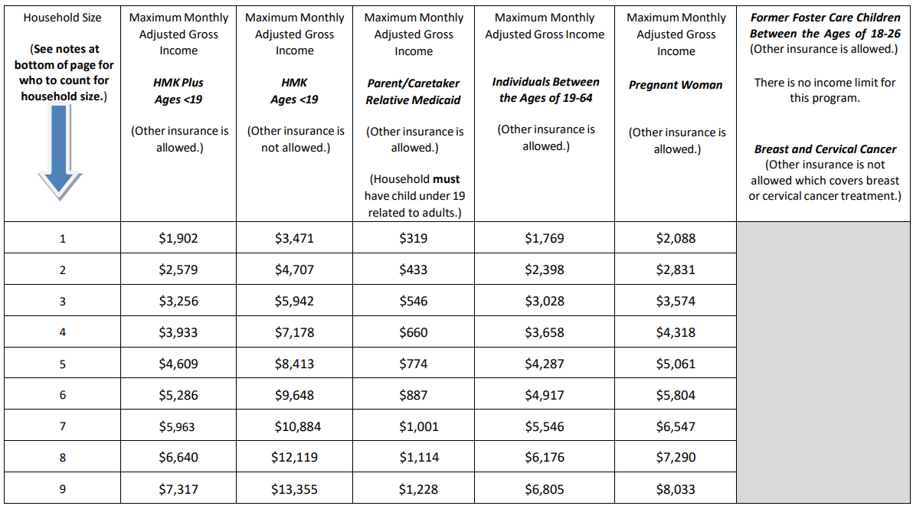
The Income Calculation Tool is updated annually to reflect changes to the Federal Poverty Level.
Step 4 – Evaluate for Community Engagement Requirements
Starting July 1, 2026 QE's must assess for Community Engagement requirements for applicants who may qualify under the Medicaid Expansion group.
When completing the PE application:
1) Determine whether the applicant is eligible for Medicaid Expansion coverage
- QEs should determine whether or not the applicant is eligible under the Medicaid Expansion group. An individual would be considered eligible under the Medicaid Expansion group if they are:
- Ages 19 – 64
- With a household income of up to 138% of the Federal Poverty Line (FPL).
- This means that applicants with a household income at or under the eligible income for their household size for Individuals Between the Ages of 19-64 in the “Current Income Calculation Tool” are required to meet community engagement requirements.
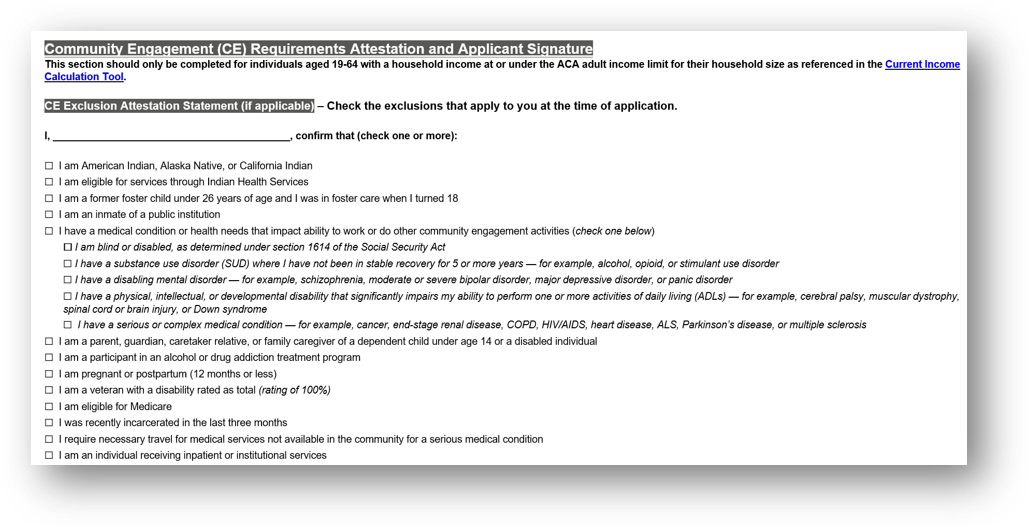
2) Assess whether the applicant qualifies for a Community Engagement exclusion
- Applicants eligible for Presumptive Eligibility under the following groups are considered excluded from having to meet community engagement requirements:
- Children (HMK Plus and HMK)
- Parent/Caretaker Relative Medicaid
- Former Foster Care Children (ages 18 up to 26
- Pregnant Women (Ambulatory Prenatal Care)
- Breast and Cervical Cancer (under age 65)
- Applicants not in the above groups may qualify for additional exclusions not listed above.
- Applicants who qualify for an exclusion must attest to being a part of the excluded group at application.
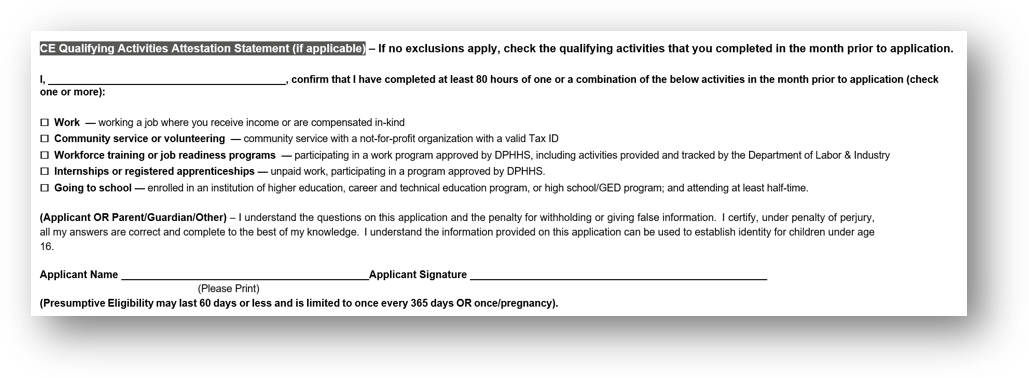
3) If no exclusion applies, assess if the applicant meets Community Engagement requirements the month prior to application
- If an applicant is unable to attest to qualifying for an exclusion, the applicant must attest to completing 80 hours of qualifying activities in the month prior to application
- If an applicant is unable to attest to completing the qualifying activities, the applicant is considered non-compliant with community engagement requirements.
4) Document the application’s responses and complete all required sections of the PE application before submitting the Proof of Temporary Coverage form.
Note: During the Hold Harmless period (July – September 2026), applicants will be evaluated for Community Engagement requirements, but otherwise eligible applicants will not be denied coverage for noncompliance. Beginning October 2026, Community Engagement requirements will be fully enforced.
A new section has been added to the PE application to document attestation to an exclusion and/or qualifying activities.
Step 5 – Finalizing the PE Process
After completion of the PE application QE’s must:
• Review the PE application to be sure the applicant completed all fields
• Review the “For Office Use Only” section to assure all fields are completed
• Evaluate whether the applicant qualifies for a Community Engagement exclusion or attests to meeting Community Engagement requirements, if applicable.
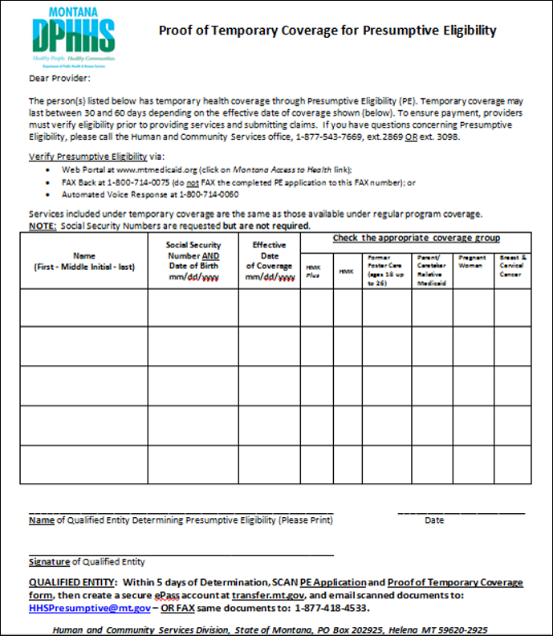
• Complete the Proof of Temporary Coverage Form
• Make Copies of the PE application AND the proof of Temporary Coverage for the applicant
Provide Proof of Temporary Coverage
• Provide the applicant with a completed Proof of Temporary Coverage form, which serves as temporary proof of PE coverage until a member ID card is issued.
Step 6 – Follow Up and Scan/Fax
- Explain that the applicant will receive additional eligibility information from DPHHS.
- Direct the applicant to available online resources for information about their Medicaid benefits and coverage.
- medicaid.mt.gov/memberguide.pdf -- use for HMK Plus (Children’s Medicaid), Parent/ Caretaker Relative Medicaid, Former Foster Care, Pregnant Woman, and Breast & Cervical Cancer benefit information
- http://hmk.mt.gov/hmkresources.shtml (click on HMK Member Handbook) -- use for Healthy Montana Kids (CHIP) benefit information.
!!!Important!!! Further Application Assistance required!
- Inform the applicant they will receive a letter within approximately 10 days confirming their PE enrollment.
- Provide the applicant with an Application for Health Coverage and explain that it must be completed to be considered for ongoing Medicaid coverage.
- Assist or refer them to the appropriate contact in your facility who will assist them with completing the application, gathering any needed verifications, AND submitting the “Application for Health Coverage” to the State of Montana.
- Reinforce that the PE application is the first step in applying for on-going coverage, and they may be contacted if additional information is related to Community Engagement requirements or exclusions, if applicable.
Scan or Fax
Within 5 days of the date of determination, Scan the PE Application, and Proof of Temporary Coverage form, create a secure ePass account (Web address: transfer.mt.gov), and email the scanned documents to: HHSPresumptive@mt.gov OR fax the application and Proof of Temporary Coverage form to Central Office at 1-877-418-4533
Keep a copy of your email with SCANNED documents attached, OR your FAX verification sheet with all faxed materials, in the event the State does not receive them. You should receive a faxed copy of the State’s applicant enrollment letter within ten days. If you do not receive the letter, call Central Office at 877-543-7669 to confirm whether your SCAN or FAX was received and processed.
Summary of Qualified Entity Responsibilities
Remember, PE Coverage begins on the Determination Date.
- As soon as possible after a person presents for services, determine if they are uninsured or underinsured. Check the Web Portal to determine if the person already has or has had PE within the past 12 months, or if coverage already exists. If the person has existing coverage, or has had PE within the past 12 months, STOP! No further action is necessary.
- You can help the client apply for Health Coverage using the Application for Health coverage and Help Paying Costs, if the client wants your help.
2. Provide the PE Application for completion by the client.
- Make sure they sign the application.
3. Complete the appropriate QE boxes/information on the PE Application AND the Proof of Coverage form.
4. Finalize your determination after evaluating income based on the household size.
- Be sure the use the Income Tool to determine eligibility with the household’s income. It is very important that the client be determined eligible or not eligible correctly.
5. Sign and date the application after all the information requested on the form has been completed.
6. Give the applicant a copy of the completed PE application, the completed Proof of Temporary Coverage letter, and the Application for Health Coverage and Help Paying Costs.
- Be sure to arrange for assistance with completion of the form and gathering of needed information. Assist with submission for the State of Montana for eligibility determination.
7. Fax or scan the completed PE Application and Proof of Temporary coverage form to Central office within 5 days of the date of determination.
- Fax number is 1-877-418-4533
Please contact us at any time if you have questions, need training or additional supplies, or need to verify any information about presumptive eligibility.
Return to the Presumptive Eligibility Page
Index
In place of an index, this edition has three search options.
- Search the whole manual. Open the Complete Manual tab. From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials".) The search box will show all locations where denials are discussed in the manual.
- Search by chapter. Open any chapter tab (for example the "Billing Procedures" tab). From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials".) The search box will show where denials are discussed in just that chapter.
- Site search. Search the manual as well as other documents related to a particular search term on the Montana Healthcare Programs site specific search page.
End of Presumptive Eligibility Guide
Update Log
Publication History
This publication supersedes all previous Presumptive Eligibility . Published by the Montana Department of Public Health & Human Services, July 2016 and prior. This manual was updated June 2017.
CPT codes, descriptions and other data only are copyright 2014 American Medical Association (or such other date of publication of CPT). All Rights reserved. Applicable FARS/DFARS Apply.
Update Log
06/152017 The manual was updated to include 2017 requirements and converted to a 508 compliant format.
Table of Contents
Presumptive Eligibility Public Assistance Programs
Key Contacts
Definitions
The Role of a Qualified Entity
Eligibility and Coverage
Timing
Step 1 – Verify the Person(s) Coverage Status
Step 2 – The Presumptive Eligibility Application
Applicant Information
Household Information
Income Information and Signature
Application Addendum for Immigrants (Information on Qualified Non-Citizens)
QE Evaluates Who Counts in Household Size
Step 3 – Making a PE Determination
Step 4 – Evaluate for Community Engagement Requirements
Step 5 – Finalizing the PE Process
Provide Applicant with Information and Proof of Temporary Coverage
Step 6 – Follow Up and Scan/Fax
Summary of Qualified Entity Responsibilities
Index
Presumptive Eligibility Public Assistance Programs
Beginning January 1, 2014, hospitals and other designated facilities participating with Medicaid can offer Presumptive Eligibility (PE) to additional coverage groups.
Note: Prior to 2014, PE was available only for children and pregnant women. PE is now available for additional Medicaid coverage groups for individuals who meet eligibility requirements. The following Medicaid coverage groups may receive Presumptive Eligibility if they meet eligibility requirements.
All providers electing PE must comply with State of Montana requirements for determining PE for the following groups:
► HMK Plus, formerly known as Children’s Medicaid
- Children 0 up to age 19
- Income limits up to 143% Federal Poverty Level
- Children may have primary insurance and still qualify for HMK Plus
► HMK, formerly known as Children’s Health Insurance Program (CHIP)
- Children 0 up to age 19
- Income limits up to 261% Federal Poverty Level
- Applicants CANNOT have other health insurance and receive HMK
► Parent/Caretaker Relative (Medicaid)
- For individuals who live together and are related by Marriage and/or Parentage.
- The parent or caretaker relative must have a related dependent child under age 19 living with them in the home to be eligible.
► Pregnant Woman
- Must be pregnant at the time of application and have income at or below 157% of the FPL
- A pregnant woman may be eligible for PE more than once in 12 months if they are pregnant more than once in that 12- month period
- For Pregnant women presenting for services prior to delivery
- See Income Calculation Tool for Household Income levels
► Individuals age 19-64 (Medicaid Expansion)
- For individuals between the ages of 19-64.
- Not pregnant at the time of application.
- Not eligible for or enrolled in Medicare Part A
- Not enrolled in Medicare Part B
- For parents and caretakers not income eligible for the Parent/Caretaker Relative Medicaid.
- Individuals may need to be evaluated for Community Engagement requirements if they meet Medicaid Expansion eligibility criteria, and do not qualify for an exclusion.
► Former Foster Care (Medicaid)
- Adults 19 up to 26
- For individuals who were in Foster Care and receiving Medicaid when they turned 18
- No income limit or resource/asset test
- Should be evaluated for PE as an individual even if living in a household with other family member
► Breast and Cervical Cancer
- For woman (ages 19 through 64) presenting for services after screening at a designated Montana Breast and Cervical Health Program facility AND after receiving diagnosis and treatment options for breast and/or cervical cancer.
- The following forms must be presented to be eligible for PE:
- Montana Breast and Cervical Screening Form
- Enrollment Form, and
- Montana Breast and Cervical Cancer Treatment Program Medicaid Referral
- Income and household size do not need to be evaluated for PE since they are reviewed during the Breast and Cervical Cancer Screening process.
- Applicants cannot have other insurance which covers breast or cervical cancer treatment.
Benefits for each of these groups vary according to the coverage group. Presumptive eligibility provides immediate, temporary health coverage for eligible individuals. Recipients are allowed ONE PE period every 12 months (dated from the most recent PE effective date) OR once per pregnancy. (A pregnant woman may be eligible more than once in 12 months if they have more than one pregnancy during that 12-month period).
Definitions:
Applicant:
Person applying for coverage for themselves, a spouse, or dependent child
Application:
The Presumptive Eligibility Application
Application for Health Coverage:
The “Application for Health Coverage & Help Paying Costs” used to apply for ongoing health coverage for Medicaid, HMK, or HMK Plus. Appendices A, B, or C may need to be completed if they apply.
Breast and Cervical Cancer:
Women ages 19 through 64 who have been screened and diagnosed with breast or cervical cancer; applicants must present 3 required forms and must not have other insurance which covers cancer treatment.
Determination:
Eligibility decision for Presumptive Eligibility (PE) coverage.
Determination Date:
The date a presumptive eligibility decision is made by a Qualified Entity (QE).
Eligibility Period:
Presumptive Eligibility coverage starts on the date of determination and ends the earlier of: the date a determination of ongoing program eligibility is made, or the end of the month following the month of the PE determination. An applicant may have only one PE period in 12 months, or only one PE Period per pregnancy.
Federal Poverty Level (FPL):
Poverty guidelines for the 48 contiguous stated and the District of Columbia as published under the “Annual Update on HHS Poverty Guidelines” in the Federal Register each year, on or about February 15. The FPL is used in combination with household size to determine presumptive eligibility.
Former Foster Care between ages 18 and 26: Individuals who were in Foster Care and receiving Medicaid when they turned 18. May apply for PE if between ages 18 and 25(until age 26), and should be evaluated for PE as an individual even if living in a household with other family members. No Income limits apply.
Health Montana Kids (HMK):
Formerly known as the "Children’s Health Insurance Plan(CHIP)", HMK serves eligible children up to age 19 in households with income between 143% and 261% of the FPL.
Health Montana Kids Plus (HMK Plus):
Formerly known as "Children’s Medicaid", HMK Plus serves eligible children up to age 19 in households with incomes between 0% and 143% of the FPL.
Income Calculation Tool:
Reference table identifying household size and corresponding maximum income levels for persons or households applying for Presumptive Eligibility.
Individuals ages 19-64:
This expansion group covers individuals ages 19-64 that are not pregnant at the time of application, not eligible for or enrolled in Medicare Part A, not enrolled in Medicare Part B and are between 24% and 133% of the FPL.
Parent/Caretaker Relative Medicaid:
For individuals living together and related by marriage and/or parentage. The parent or caretaker relative must have an eligible related dependent child under age 19 living in the home and have income between 0% and 23% of the FPL.
Pregnant Woman:
Pregnant women presenting for services prior to delivery. The income limit for this category is from 0% to 157% of the FPL. No hard copy verification of pregnancy is required. Covers ambulatory prenatal care ONLY.
PE Determination:
A decision of temporary eligibility is called a determination. A Qualified Entity (QE) from a healthcare facility must be trained by the State of Montana in order to make a PE Determination based on self-attested information provided by an individual or household.
Presumptive Eligibility (PE): Expedited eligibility process of determining temporary health care coverage for persons eligible for specific public assistance programs.
Proof of Temporary Coverage Letter:
Approval notices prepared by a QE verifying temporary coverage in a specific public assistance program; used in place of a member ID card.
Qualified Entity (QE):
Representative of a health facility trained and certified to make Presumptive Eligibility determinations.
Self-Attestation:
An applicant’s sworn statement of the accuracy of the information they provide, such as income, household size, and residency, as reported on an application or as a change either verbally, electronically, or in writing.
Web Portal:
On-Line resource site for Qualified Entities and health care providers to check current health care coverage for persons applying for PE ( access from the home page of the provider website).
The Role of a Qualified Entity
Access to health care is critical for uninsured or underinsured persons when faced with sudden, serious, and often very expensive health care needs. Qualified Entities are vital to the Presumptive Eligibility process. As a Qualified Entity, you are trained and certified to make accurate, complete and timely determinations of PE coverage. PE begins on the date a Qualified Entity makes a PE determination and continues until a complete eligibility determination is made or until the last day of the month following the month PE began, whichever occurs first. Reimbursement for your facility, and the family’s peace of mind depend upon your due diligence and attention to detail. Once you determine a person presumptively eligible, your facility’s services will be paid covered services on or after the date of your determination, and PE coverage may continue for a period up to the end of the month following the month of determination. If a PE application was turned in for a group that is not eligible for PE coverage, they would be denied, and the client would be responsible for the services they received. This is yet another reason to have the client complete a regular Medicaid application.
Eligibility and Coverage
- Presumptive Eligibility is based primarily on age, status of the applicant(s), and household size and income.
- PE Coverage is temporary – Eligibility begins on the date of determination and ends the last day of the month following the month of determination, or sooner, if a determination of ongoing program eligibility is finalized. Facilities are required to provide applicants with the Application for Coverage and Help Paying Costs and Appendices A, B, and C , and assist with the completion of applications and appendices if necessary.
- A person may have only ONE PE period in a twelve month period, OR once per pregnancy. (A pregnant woman may be eligible more than once in 12 months if they have more than one pregnancy during that 12-month period).
- Presumptively eligible persons receive the same benefits as a standard covered enrollee in the public assistance program for which they are eligible during the presumptive eligibility period. The exception to this is Pregnant Woman Presumptive, only ambulatory services are covered.
Timing
- On the date a person presents for services, or as soon as possible, have the applicant (or a representative) complete the Presumptive Eligibility Application. PE coverage begins on the date of determination. If eligible, the person has timely coverage, and the facility is reimbursed for covered services.
- The PE application AND the Proof of Temporary Coverage Form must be faxed or scanned and emailed to the Human and Community Services Central Office within 5 days of making the Presumptive Eligibility Determination. Staff will then finalize the PE enrollment so eligibility information displays correctly on the web portal to generate the appropriate reimbursement for services.
- If a PE determination cannot be made on the date a person presents for services or the first day of a hospital stay, an Application for Health Coverage and Help Paying Costs should be completed an turned in to the State (with required documentation) during the same month the person receives series. Then, pending an eligibility determination, the eligibility effective date would be the 1st of the month of application OR date of birth (for newborns).
Step 1 - Verify the Person(s) Coverage Status
* Verify if the person has current coverage and/or
* Verify if the person has received Presumptive Eligibility within the past 12 months:
► Web Portal – www.mtmedicaid.org (see “Eligibility Spans”, example below)
► Fax Back – 1-800-714-0075
► Automated Voice Response – 1-800-714-0060
Web Portal Example 1 (Verify if the person has current coverage):
Web Portal Example 2 (Verify if the person had PE within the past 12 months):
Step 2 – The Presumptive Eligibility Application
Have the Applicant (or a representative) complete the Presumptive Eligibility Application as follows:
-
Applicant and Household Non-financial Information
-
Household Information
►Page 3 of the application also includes an Addendum for immigrants who need information about whether they are a Qualified Non-Citizen. The Addendum does not need to be submitted with the PE application. See the information from the Addendum later in this chapter.
►"Has Health Insurance" applies only to those who may qualify for HMK PE
-
Income and Signature
-
Application Addendum for Immigrants (Information on Qualified Non-Citizen)
ALL PERSONS WHO ARE IMMIGRANTS NEED TO REVIEW THE FOLLOWING INFORMATION TO DETERMINE IF THEY ARE A QUALIFIED NON-CITIZEN; THEN THEY SHOULD MARK THE APPROPRIATE RESPONSE ON THE
PRESUMPTIVE ELIGIBILITY APPLICATION, HOUSEHOLD INFORMATION, COLUMN 8.
Those who are in ANY of the following groups would be considered a Qualified Non-Citizen:
- Lawful Permanent Residents (LPR/Green Card Holder ) **SEE FURTHER INFORMATION, BELOW
- Asylees
- Refugees
- Cuban/Haitian entrants
- Paroled into the U.S. for at least one year
- Conditional entrant granted before 1980
- Battered non-citizens, spouses, children, or parents
- Victims of trafficking and his or her spouse, child, sibling, or parent or individuals with a pending application for a victim of trafficking visa
- Granted withholding of deportation
- Member of a federally recognized Indian tribe or American Indian born in Canada
- Children lawfully residing in the state of Montana (lawfully present and otherwise eligible for Medicaid or HMK in the state, including being a state resident)
**In order to get Medicaid coverage, under current law most ADULT Lawful Permanent Residents or green card holders have a 5-year waiting period. This means they must wait 5 years after receiving “qualified” immigration status before being eligible for Medicaid. There are also exceptions -- Lawful Permanent Residents who don’t have to wait 5 years -- such as people who used to be refugees or asylees.
Montana has removed the 5-year waiting period to cover lawfully residing children who are otherwise eligible for Medicaid or HMK. A child is “lawfully residing” if lawfully present and otherwise eligible for Medicaid or HMK in the state (including being a state resident).
NOTE: Immigrants who are qualified non-citizens are generally eligible for Medicaid and Children’s Health Insurance Program (HMK) coverage IF they are otherwise eligible for Medicaid and HMK in the state; that is, if they meet Montana’s income eligibility rules .
-
QE Evaluates Who Counts in Household Size
Before making a PE Determination, a Qualified Entity needs to evaluate which individuals will be “counted” as part of the household. The following examples can be referenced for how to count persons in the household.
Pregnant Women: Include the pregnant woman, the unborn child(ren), the father of the unborn (if married and living together), and any other children (of the unborn’s married parents) under age 19 who live in the home. For example:
- Ann is a single mother with one child and has a significant other in the household. She is pregnant with one child. For this household,
Count: Ann, her child, and the unborn (Household Size 3). Do not count the significant other OR his income because he and Ann are not married. - Julie and her husband are expecting their first child, and are living in the same household.
Count: Julie, her husband, and the unborn (Household size 3) and all their income. - Mary and her husband have 2 children and Mary is pregnant. They currently live with Mary’s parents, who require living assistance.
Count: Mary, her husband, their 2 children and the unborn (Household size 5) and their income.
DO NOT Count Mary’s parents.
Healthy Montana Kids (HMK), Health Montana Kids Plus (HMK Plus), Parent/Caretaker Relative, and individuals between 19-64 years old: Include all those on the application that are connected by marriage or parentage who live in the household, along with any unborn children. This includes all Natural, Adoptive, and/or Step-Parents and birth, adoptive, or step-children under age 19, as well as any unborn children of these persons. DO NOT INCLUDE other adult relatives who file their own tax return. For Example:
- Pamela, her significant other Dan, Pamela’s two children, and Pamela and Dan’s unborn child all live together.
Count: Pamela, her two children, and the unborn (Household size 4).
DO NOT Count: Dan and his income until there is a child in common for him and Pamela. Once the baby is born, Count: Pamela, Dan, her two children, and Pamela and Dan’s child in common (Household Size 5), as Dan is connected by parentage. - Lily, Rose, and Paul live with their maternal grandparents and are not adopted by the grandparents.
Count: Lily, Rose, and Paul only (Household size 3).
Do Not Count: The grandparents as they are not related by parentage. - Susan has 3 children, including and 18 year old daughter who just had a baby. Susan’s brother Michael and his son also live with Susan, her children and grandchild.
Count: Susan, her children, and her grandchild (Household Size 5).
Do Not Count: Michael and his son don’t count as they are not related to Susan, her children or grandchild by marriage or parentage.
Individuals age 19-64 : Include all household members that are between the ages of 19 and 64, not pregnant at the time of application, not eligible for or enrolled in Medicare Part A or B, and Parent/Caretaker relatives that are over income for the Parent/Caretaker Relative Medicaid. For Example:
- Cindy, her significant other Jim, and her two children all live together.
Count: Cindy and her two children.(Household Size 3).
Do Not Count: Jim is his own household. Because Cindy and Jim are not married, they will not be counted in the same household. If they were married, everyone would be included (Household size 4).
Step 3 – Making a PE Determination
Qualified Entities must complete the “For Office Use only” box for ALL PE Determinations.
Complete the entire box “For Office Use Only.” Copy the “Combined Total Monthly Gross Income” figure from the applicant’s Income information box. Count how many people are in the household and record the number under “Household Size” in the box shown above. Compare Combined Total Monthly Gross Income to Current Income Calculation Tool based on household size for the program being considered for each individual.
The Income Calculation Tool is updated annually to reflect changes to the Federal Poverty Level.
Step 4 – Evaluate for Community Engagement Requirements
Starting July 1, 2026 QE's must assess for Community Engagement requirements for applicants who may qualify under the Medicaid Expansion group.
When completing the PE application:
1) Determine whether the applicant is eligible for Medicaid Expansion coverage
- QEs should determine whether or not the applicant is eligible under the Medicaid Expansion group. An individual would be considered eligible under the Medicaid Expansion group if they are:
- Ages 19 – 64
- With a household income of up to 138% of the Federal Poverty Line (FPL).
- This means that applicants with a household income at or under the eligible income for their household size for Individuals Between the Ages of 19-64 in the “Current Income Calculation Tool” are required to meet community engagement requirements.
2) Assess whether the applicant qualifies for a Community Engagement exclusion
- Applicants eligible for Presumptive Eligibility under the following groups are considered excluded from having to meet community engagement requirements:
- Children (HMK Plus and HMK)
- Parent/Caretaker Relative Medicaid
- Former Foster Care Children (ages 18 up to 26
- Pregnant Women (Ambulatory Prenatal Care)
- Breast and Cervical Cancer (under age 65)
- Applicants not in the above groups may qualify for additional exclusions not listed above.
- Applicants who qualify for an exclusion must attest to being a part of the excluded group at application.
3) If no exclusion applies, assess if the applicant meets Community Engagement requirements the month prior to application
- If an applicant is unable to attest to qualifying for an exclusion, the applicant must attest to completing 80 hours of qualifying activities in the month prior to application
- If an applicant is unable to attest to completing the qualifying activities, the applicant is considered non-compliant with community engagement requirements.
4) Document the application’s responses and complete all required sections of the PE application before submitting the Proof of Temporary Coverage form.
Note: During the Hold Harmless period (July – September 2026), applicants will be evaluated for Community Engagement requirements, but otherwise eligible applicants will not be denied coverage for noncompliance. Beginning October 2026, Community Engagement requirements will be fully enforced.
A new section has been added to the PE application to document attestation to an exclusion and/or qualifying activities.
Step 5 – Finalizing the PE Process
After completion of the PE application QE’s must:
• Review the PE application to be sure the applicant completed all fields
• Review the “For Office Use Only” section to assure all fields are completed
• Evaluate whether the applicant qualifies for a Community Engagement exclusion or attests to meeting Community Engagement requirements, if applicable.
• Complete the Proof of Temporary Coverage Form
• Make Copies of the PE application AND the proof of Temporary Coverage for the applicant
Provide Proof of Temporary Coverage
• Provide the applicant with a completed Proof of Temporary Coverage form, which serves as temporary proof of PE coverage until a member ID card is issued.
Step 6 – Follow Up and Scan/Fax
- Explain that the applicant will receive additional eligibility information from DPHHS.
- Direct the applicant to available online resources for information about their Medicaid benefits and coverage.
- medicaid.mt.gov/memberguide.pdf -- use for HMK Plus (Children’s Medicaid), Parent/ Caretaker Relative Medicaid, Former Foster Care, Pregnant Woman, and Breast & Cervical Cancer benefit information
- http://hmk.mt.gov/hmkresources.shtml (click on HMK Member Handbook) -- use for Healthy Montana Kids (CHIP) benefit information.
!!!Important!!! Further Application Assistance required!
- Inform the applicant they will receive a letter within approximately 10 days confirming their PE enrollment.
- Provide the applicant with an Application for Health Coverage and explain that it must be completed to be considered for ongoing Medicaid coverage.
- Assist or refer them to the appropriate contact in your facility who will assist them with completing the application, gathering any needed verifications, AND submitting the “Application for Health Coverage” to the State of Montana.
- Reinforce that the PE application is the first step in applying for on-going coverage, and they may be contacted if additional information is related to Community Engagement requirements or exclusions, if applicable.
Scan or Fax
Within 5 days of the date of determination, Scan the PE Application, and Proof of Temporary Coverage form, create a secure ePass account (Web address: transfer.mt.gov), and email the scanned documents to: HHSPresumptive@mt.gov OR fax the application and Proof of Temporary Coverage form to Central Office at 1-877-418-4533
Keep a copy of your email with SCANNED documents attached, OR your FAX verification sheet with all faxed materials, in the event the State does not receive them. You should receive a faxed copy of the State’s applicant enrollment letter within ten days. If you do not receive the letter, call Central Office at 877-543-7669 to confirm whether your SCAN or FAX was received and processed.
Summary of Qualified Entity Responsibilities
Remember, PE Coverage begins on the Determination Date.
- As soon as possible after a person presents for services, determine if they are uninsured or underinsured. Check the Web Portal to determine if the person already has or has had PE within the past 12 months, or if coverage already exists. If the person has existing coverage, or has had PE within the past 12 months, STOP! No further action is necessary.
- You can help the client apply for Health Coverage using the Application for Health coverage and Help Paying Costs, if the client wants your help.
2. Provide the PE Application for completion by the client.
- Make sure they sign the application.
3. Complete the appropriate QE boxes/information on the PE Application AND the Proof of Coverage form.
4. Finalize your determination after evaluating income based on the household size.
- Be sure the use the Income Tool to determine eligibility with the household’s income. It is very important that the client be determined eligible or not eligible correctly.
5. Sign and date the application after all the information requested on the form has been completed.
6. Give the applicant a copy of the completed PE application, the completed Proof of Temporary Coverage letter, and the Application for Health Coverage and Help Paying Costs.
- Be sure to arrange for assistance with completion of the form and gathering of needed information. Assist with submission for the State of Montana for eligibility determination.
7. Fax or scan the completed PE Application and Proof of Temporary coverage form to Central office within 5 days of the date of determination.
- Fax number is 1-877-418-4533
Please contact us at any time if you have questions, need training or additional supplies, or need to verify any information about presumptive eligibility.
Return to the Presumptive Eligibility Page
Index
This edition has three search options.
- Search the whole manual. Open the Complete Manual tab. From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials".) The search box will show all locations where denials are discussed in the manual.
- Search by chapter. Open any chapter tab (for example the "Billing Procedures" tab). From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials".)The search box will show where denials are discussed in just that chapter.
- Site Search. Search the manual as well as other documents related to a particular search term on the Montana Healthcare Programs site specific search page.
End of Index Chapter
End of Presumptive Eligibility Guide